Exercise 5: The Appendicular Skeleton
Figure 5.1 This statue exemplifies the importance of the appendicular skeleton and joints in body movement.
Exercise 5 Learning Goals After completing this lab, you should be able to:
- Label and identify different structures associated with bone histology
- Explain the difference between compact and spongy bone
- Recognize and define parts of long bones
- Identify bones of the appendicular skeleton
- Identify bone marking associated with appendicular bones
Pre-Lab Activities for Exercise 5Pre-Lab Activity 5.1: Parts of Long Bones
We think of bones as hard, rigid nonliving tissue because we examine this unique connective tissue postmortem. Bone is a dynamic living tissue in the human body that provides structural support and protects important soft tissues. Describe the following external features of long bone and locate them from the lettered image from the next page.
Feature | Description | Function | Letter |
Diaphysis | The long cylindrical center shaft of a long bone | Forms the medullary cavity where bone marrow is found | |
Epiphysis (Proximal and distal) | |||
Metaphysis | |||
Articular Cartilage | |||
Periosteum | |||
Medullary Cavity | |||
Endosteum | |||
Epiphyseal plate/line | |||
Nutrient artery | |||
Compact bone | |||
Cancellous/ Trabecular bone | |||
Red bone marrow | |||
Yellow bone marrow |
Figure 5.2 Long bone features.
Pre-Lab Activity 5.2: Appendicular Skeleton
The appendicular skeleton connects the upper and lower limbs to the axial skeleton via the shoulder and pelvic girdles. In this lab, you will learn not only the names of these bones, but how they articulate with one another and the bony landmarks that reside on them. Familiarize yourself with the bones below and how they articulate with one another. Complete the table below describing the shape of each bone and how each contributes to movement.
Bone(s) | Articulates with... | Shape |
Clavicle | Scapula and sternum | S-shaped |
Scapula | ||
Humerus | ||
Radius | ||
Ulna | ||
Carpals | ||
Metacarpals | ||
Phalanges of the Hand | ||
Ilium | ||
Ischium | ||
Pubis | ||
Femur | ||
Tibia | ||
Fibula | ||
Tarsals | ||
Metatarsal | ||
Phalanges of the Foot | ||
Patella |
Figure 5.3: Demonstrating bones of the skeletal system
Exercise 5: Appendicular Skeleton
Activity 5.1: Bone Histology
The skeletal system supports soft tissue, protects delicate organs, and works with muscles to generate movements. Bone forms through two mechanisms of ossification, intramembranous and endochondral. Intramembranous ossification means bone forms within the mesenchymal member, which is how skull and facial bones are formed. Endochondral ossification is the formation of bones from an original cartilage model, and this is how long bones are formed. Bone is characterized as compact or spongy bone and depending on whether there is extra space withing the extracellular matrix. The structural unit for compact bone is the osteon and for spongy bone it is known as trabeculae. Each osteon of bone is composed of basic parts: lamellae, lacunae, canaliculi, central canal osteoblasts and osteocytes. Lamellae are circular rings of extracellular matrix composed of collagen and mineral salts giving bone strength. Lacunae are small spaces filled with fluid where osteocytes live. Canaliculi are processes radiating from the lacuna, providing nutrients, and removing wastes from osteocytes. The central canal contains the blood vessels and nerves connecting bone to the other structures. Osteocytes are mature bone cells that get trapped in the extracellular matrix and osteoblast are immature cells that lay down collagen and initially form the extracellular matrix during ossification.
Using the 10X and/or 40X objectives on your microscope, examine a section of compact bone and identify the following structures:
- Osteon
- Lacuna
- Interstitial lamellae
- Concentric lamellae
- Canaliculi
- Osteocyte
Figure 5.4: Diagram of compact bone.
Activity 5.2: Pectoral Girdle
The pectoral (shoulder) girdle is composed of two bones, the clavicle and scapula, which together function as the proximal attachment points for the arms to the axial skeleton. The head of the humerus (arm) articulates with the shallow glenoid cavity of the scapula. This design sacrifices stability for increased mobility at the shoulder girdle.
On a bone model label the clavicle and the scapula including specific features listed below
Clavicle (right and left)
- Acromial end
- Sternal end
- Conoid tubercle
Scapula (right and left)
- Acromion
- Spine
- Glenoid cavity
- Coracoid process
Figure 5.5: Pectoral girdle and clavicle
Activity 5.3: Scapula and Clavicle
Using a disarticulated skeleton in the lab, learn how to differentiate the anterior from posterior surface of the clavicle and scapula.
Figure 5.6 Scapula and associated markings
Activity 5.4: Bones of the Arm
The humerus is a long bone that articulates proximally with the glenoid cavity of the scapula and distally with the radius and ulna. It is the longest and largest bone of the upper limbs. The radius is the smaller lateral bone of the forearm articulating with the capitulum proximally and the carpal bones distally. The ulna is the medial bone of the forearm which articulates with the trochlea proximally and the carpal bones distally. Identify and label the humerus, radius and ulna including landmarks.
 Identify each bone of the arm and its specific markings. Using the disarticulated skeleton in the lab, to identify the anterior from posterior surface of each bone.
Identify each bone of the arm and its specific markings. Using the disarticulated skeleton in the lab, to identify the anterior from posterior surface of each bone.
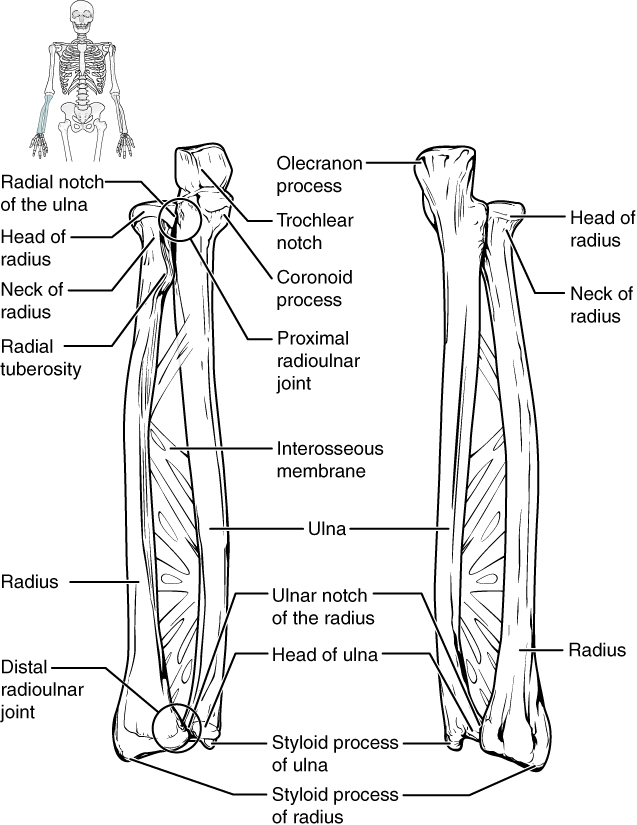
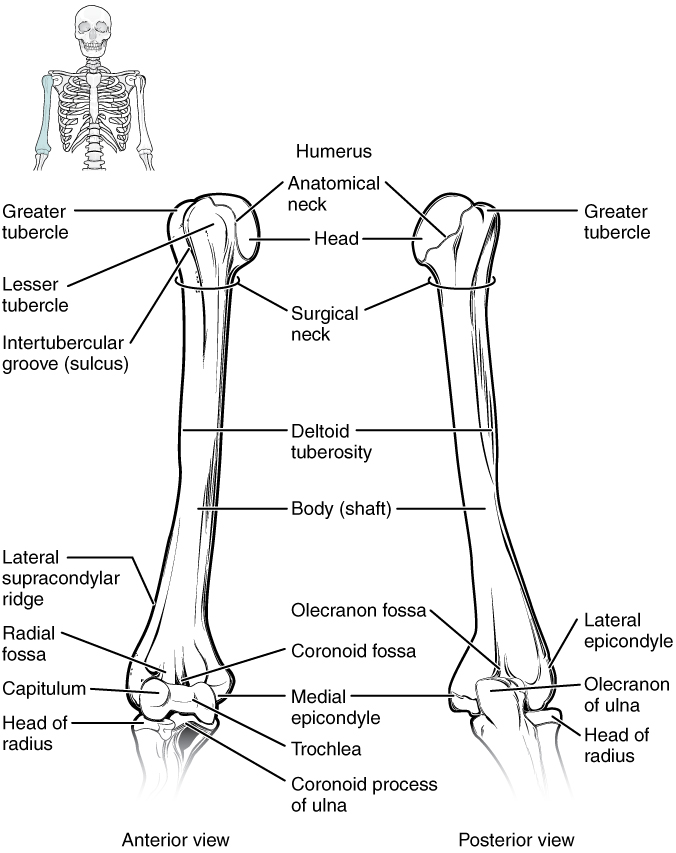
Figure 5.7 Humerus, radius, and ulna along with associated markings
Humerus (right and left)
- Head
- Greater tubercle
- Surgical neck
- Intertubercular sulcus
- Deltoid tuberosity
- Lateral and Medial Epicondyles
- Trochlea
- Capitulum
- Olecranon fossa
Radius (right and left)
- Head
- Radial Tuberosity
- Interosseus membrane
Ulna (right and left)
- Olecranon process
- Trochlear notch
- Radial notch
- Head
Activity 5.5: Bones of the Wrist and Hand
The bones of the wrist are collectively known as carpal bones and these eight short bones are held together by ligaments. The bones are arranged in two rows of four bones. The proximal row from lateral to medial includes the scaphoid (boat-shaped), lunate (moon-shaped), triquetrum (three-cornered), and pisiform (shaped like a pea). The distal row from lateral to medial includes the trapezium (four-sided), trapezoid (four-sided), capitate (shaped like a head), and hamate (hook-shaped).
Figure 5.8 Carpals, metacarpals, and phalanges
Locate the carpal bones using the hand on the whole skeleton. Note how they articulate with the bones of the arm and the metacarpals.
- What bones are immediately proximal to the carpals?
- What bones are distal to the carpals?
Five metacarpals form the palm of the hand. These long bones articulate with the proximal phalanx. The metacarpal bones do not have specific names but are labeled 1-5 (I-V) from lateral to medial in anatomical position. Identify the following features of the metacarpal bones: Base, shaft, and head.
The phalanges are the long bones that make up the digits on each hand. The 4 fingers are composed of a proximal, middle, and distal phalanx. The pollex (thumb) is only composed of a proximal and distal phalanx.
- Identify the proximal, middle, and distal phalanx for each digit
- Identify the pollex: proximal and distal phalanx
Figure 5.9 Pelvic girdle and associated markings
Activity 5.6: Pelvic Girdle
Formed by the union of the two hip bones (os coxa) anteriorly at the pubic symphysis and posteriorly to the sacrum and coccyx, the pelvis is a strong, stable structure built for a lifetime of load bearing. The pelvic girdle, much like the shoulder girdle, is designed for the support and attachment of limbs to the body, specifically the lower limbs. By uniting with the sacral portion of the vertebral column to the coxal bones, the weight of the trunk and upper limbs can be shifted onto either lower limb simultaneously, such as when standing, or walking.
The pelvis is divided into two regions: the true pelvis and false pelvis. From the top of the pelvic brim or pelvic inlet to the superior point of the hip bone is the false pelvis or greater pelvis. The term ‘false’ is applied to this space because it does not contain pelvic organs, but rather portions of the lower abdominal organs. Below the pelvic brim extending to the pelvic outlet, is the smaller true pelvis, known as the lesser pelvis. One method of determining the sex of a skeleton in forensic bone analysis is identifying the unique characteristics of the female versus male pelvis. As shown in the figure below, the pelvic brim is wider and shallower in the female compared to males, which have a significantly narrower and more circular pelvic brim. The shape of the female pelvis allows for the distribution of weight when carrying a fetus during pregnancy and passage of the infant’s head during childbirth. Finally, the inferior angle formed by the attachment of the pubic bones to one another at the pubic symphysis is the subpubic angle or pubic arch. In women this angle is typically 90°, although it may vary from 70-90°. For men, this range is lower, typically 50-80°.
Figure 5.10 Male vs female pelvic girdle
- What features are distinct to the female pelvis?
- What features are distinct to the male pelvis?
Identify and label the bones/structures which make up the pelvis and pelvic girdle using the whole skeleton.
Is this a male or female pelvis? ____________________ |
|
Activity 5.7: Hip: Ilium, Ischium, and Pubis
The right and left os coxa (hip bone; coxal bone) are formed by three separate bones which fuse during early adulthood. In the mature adult skeleton, the os coxa retain their original unfused designations despite being one structure. Superiorly, the ilium of the os coxa has a distinctive upper ridged portion called the iliac crest formed by the wing of the ilium (or ala). The ilium joins posteriorly with the sacrum, right and left, forming the sacroiliac joint. This is frequently the site of low back pain in pregnant and older women due to hormonal effects on the ligaments stabilizing the joint. Adjacent to the sacroiliac joint on either side is the iliac tuberosity, a roughened site of muscle and ligament attachment. The posterior portion of the ilium features a deep notch below its inferior spine called the greater sciatic notch, where the sciatic nerve passes through. Joining with the ilium inferiorly and posteriorly is the ischium (seat bone), identified by a thick body and large, curving ischial ramus. The obturator foramen is formed by the medial aspect of the ischium.
The superomedial and inferomedial portions of the ischium join with the third bone of the os coxa, the pubis, to form the remaining portion of the acetabulum and the ischiopubic ramus, respectively. The anterior portion of each pubis joins at their articular surfaces to form the pubic symphysis. The lateral aspects of the superior and inferior pubic rami form the remaining circumference of the obturator foramen.
Figure 5.12 Lateral and medial view of the coxal bone
Examine the right and left coxal bones from the disarticulated skeleton and identify the following:
Ilium (R&L) | Ischium (R&L) | Pubis (R&L) |
Iliac crest | Ischial spine | Articular surface of the |
Ala | Lesser sciatic notch | Pubic symphysis |
Greater sciatic notch | Acetabulum | Acetabulum |
Acetabulum |
Activity 5.8: Bone of the Thigh
The upper portion of the lower limb, called the thigh, contains only one bone, the femur. Since the femur has no additional bony support from the hip to the knee joint, it is the single strongest bone found in the human body. Additionally, the femur typically contributes to more than 25% of an individual’s height. Thus, it is the only bone which can consistently and reliably be used to determine the height of a partial skeleton. This exceptionally large bone is divided into three main regions: the proximal end, the body (shaft), and distal end. The proximal end of the femur articulates with the acetabulum of the hip bone. Additional cartilaginous structures surround the acetabulum, deepening its cup-like shape to securely hold the head of the femur. This deep, well-protected joint is why the hip is so strong and difficult to dislocate, unlike the shoulder. The medial surface of the femoral head has a marked indentation called the fovea capitis where an artery supplying the femoral head enters. The fovea capitis is also the only surface of the femoral head not covered in hyaline cartilage. The common site of hip fracture is a narrowed region of the femur called the neck.
The neck supports the femoral head and follows a slight lateral angle which connects to the long, narrow body or shaft of the femur. Found proximally on the lateral and posterior aspects of the neck are eminences of bone called the greater and lesser trochanters, specific to only the femur. The larger, and therefore greater trochanter is a site for muscle attachment and located directly opposite the femoral head. With portions beginning below both the greater and lesser trochanter, the roughened and slightly raised ridge of the Linea aspera runs longitudinally down the posterior aspect of the femur shaft.
Figure 5.13 Femur, fibula, and tibia along with associated markings
Emerging distally from the shaft of the femur are two large eminences, the lateral and medial condyles which form the superior articular structures of the knee (tibiofemoral joint). The shape of the condyles increases the size of the femur in either direction. The roughened spots immediately superior to each condyle are the lateral and medial epicondyles, which provide attachment points for several muscles and ligaments integral to knee stability. Anteriorly, the space between the condyles forms the patellar surface which articulates with the kneecap or patella.
Identify and label the specific bone markings of the femur.
Femur (R & L) |
|
|
|
Using the disarticulated skeleton in lab, learn how to differentiate the anterior from posterior surface of the femur.
Activity 5.9 Kneecap-Patella
The best known and largest sesamoid bone in the body, the patella or kneecap, is found embedded in the large tendon of the quadriceps femoris group. The patella is a cartilaginous structure in infants and does not typically begin to ossify until early adolescence. It articulates with the anterior portion of the distal femur only (patellofemoral joint) and not the tibia.
Figure 5.14 Anterior and posterior views of patella below: Line drawing by Kingsley Dunkley
Identify the patella and learn how to differentiate the anterior from posterior surface.
Activity 5.10: Bones of the Leg
Beginning at the largest joint in the body, the knee, and extending inferiorly to the ankle, the tibia (shin bone) is the primary weight bearing structure of the lower leg and second longest bone in the body. It articulates with the smaller, non-weight bearing bone called the fibula at two tibiofibular joints, one proximal and one distal. The proximal end of the tibia expands to flattened medial and lateral condyles. The space between the condyles, the intercondylar eminence, is the site of attachment for supporting ligaments of the knee. Anteriorly, the proximal tibia features an oval protuberance called the tibial tuberosity, where the patellar ligament inserts. This “bump” can be palpated through the skin immediately below the knee joint. The portion of the leg often referred to as the “shin” is the anterior crest of the tibial shaft, felt just below the skin continuing down to the ankle. Moving from the tibial tuberosity inferiorly, the shaft of the tibia narrows significantly. At its distal end, the tibia widens slightly to form articular structures at the ankle. The tibia forms a prominent bony projection on the medial aspect of the ankle aptly named the medial malleolus. Both the distal surface of the tibia and inner surface of its medial malleolus form part of the ankle joint with a tarsal bone. Laterally, the distal tibia articulates with the distal fibula in an indentation called the fibular notch which forms the distal tibiofibular joint.
Located along the lateral side of the lower leg, the fibula is not a weight-bearing structure but rather serves as a point of muscular attachments and provides stability to the lower leg. The proximal articulating end is called the head followed by a thin shaft. The distal end forms the lateral malleolus, felt as a bony protuberance on the lateral aspect of the ankle.
Identify and label the specific leg bones and their surface markings.
Figure 5.15 Anterior and posterior views of the fibula and tibia
Tibia (R & L) | |||||||
| |||||||
| |||||||
| |||||||
| |||||||
|
Using the disarticulated skeleton in the lab, learn how to differentiate the anterior from posterior surface of each bone.
5.11: Bones of the Ankle and Foot
The foot is formed by a combination of seven tarsal bones, five metatarsals, and 14 phalangeal bones. The tarsal bone responsible for forming the distal portion of the ankle joint is the talus. The talus is the most superior tarsal bone and has three articular surfaces interacting with the tibia and fibula. The inferior aspect of the talus articulates with the largest tarsal bone, the calcaneus (heel bone). The calcaneus is the bone responsible for supporting the weight of the entire body. Articulating anteriorly with the calcaneus and talus are the cuboid and navicular bones, respectively. Anterior to the navicular are three cuneiform bones (medial, intermediate, and lateral). The superior aspect of these bones is noticeably wider than their inferior surfaces, lending themselves to the shape of the foot arch (transverse curvature).
Identify the tarsal bones as a group on an articulated skeleton of the foot.
- Locate all the tarsal bones on the skeleton
- Identify the talus and calcaneus on the models
Figure 5.16 Tarsal, metatarsals and phalanges
- What proximal bones articulate with the talus?
Connecting the tarsals to the toes (phalanges) are the five metatarsal bones (I-V). Just like the metacarpals of the hand they are numbered 1-5; however, they are ordered from medial to lateral (big toe to little toe). The proximal end of each metacarpal is known as the base and its distal end is the head. It is the metatarsal heads which form the ball of the foot.
Articulating with the metatarsals are the phalanges. Just as with the phalanges of the hand, the toes are formed by 14 different phalangeal bones. The big toe or hallux is made from two bones, a proximal and distal phalange. Toes 2-5 are formed by three phalangeal bones each, a proximal, middle, and distal.
- Identify the proximal, middle, and distal phalanx
- Identify the hallux: proximal and distal phalanx
Post-Lab 5 Review
Complete the missing information for each table. These are the bones and markings you will be expected to identify.
Upper Limb | |||||
Bones | Features to identify | Associated Joints | |||
Clavicle (L&R) | Sternal end Acromial end Conoid tubercle | ||||
(L&R) | Spine of scapula Acromion Coracoid process Glenoid cavity | ||||
(L&R) | Head Surgical neck Intertubercular sulcus Greater tubercle Deltoid tuberosity Medial epicondyle Lateral epicondyle Trochlea Capitulum Olecranon fossa | ||||
(L&R) | Olecranon Trochlear notch Radial notch Head | ||||
(L&R) | Head Radial tuberosity | ||||
Carpals | Right hand vs. Left hand | ||||
I-V | |||||
Phalanges of Hand | Proximal, Middle, Distal | ||||
| |||||
Bones | Features to identify | Associated Joints | |||
Os coxa (R&L) | Iliac Crest Greater sciatic notch Ala Acetabulum Obturator foramen | ||||
Ischial spine Ischial tuberosity Acetabulum Obturator foramen | |||||
Pubis | |||||
(R&L) | Head Neck Greater trochanter Lesser trochanter Linea aspera Medial condyle Lateral condyle | ||||
Patella (R&L) | Anterior vs. Posterior | ||||
(R&L) | Medial condyle Lateral condyle Tibial tuberosity Medial malleolus Anterior crest | ||||
(R&L) | Head Lateral malleolus | ||||
Tarsals | Right vs. Left Foot | ||||
Talus and Calcaneus | |||||
Phalanges of Feet | Proximal, Middle, Distal | ||||
Post-Lab 5 Questions
- How many total bones are in the appendicular system?
a) 100 b) 58 c) 126 d) 206
- What are the functions of the pectoral (shoulder) and pelvic girdles?
- List the specific bones and number of each that make up the upper limbs.
- List the specific bones and number of each that make up the lower limbs.
- How are metacarpals most fractured?
- How many phalanges are on each hand?
a) 7 b) 12 c) 24 d) 14
- Why is the pelvis shaped like it is? What are the main differences between the female versus male pelvis? What is the purpose for these differences?
Which bones do the tibia and fibula articulate with, proximally? Distally?
- List the ankle bones which articulate with the distal end of the tibia and fibula.
- How are metatarsals most fractured?
- How many phalanges make up each foot?
a) 7 b) 12 c) 24 d) 14
- Below is a cross section through the diaphysis of a long bone, complete the diagram by filling in the blanks.